Kyasanur Forest Disease (KFD), The Monkey Fever

Content
Why in News?
A recent fatality in Karnataka involving a 29-year-old man who contracted Kyasanur Forest Disease (KFD), commonly known as monkey fever, has once again drawn attention to this neglected but potentially deadly zoonotic disease. The incident highlights persistent gaps in surveillance, vaccination coverage, and public awareness, particularly in forest-fringe regions of southern India.
Introduction
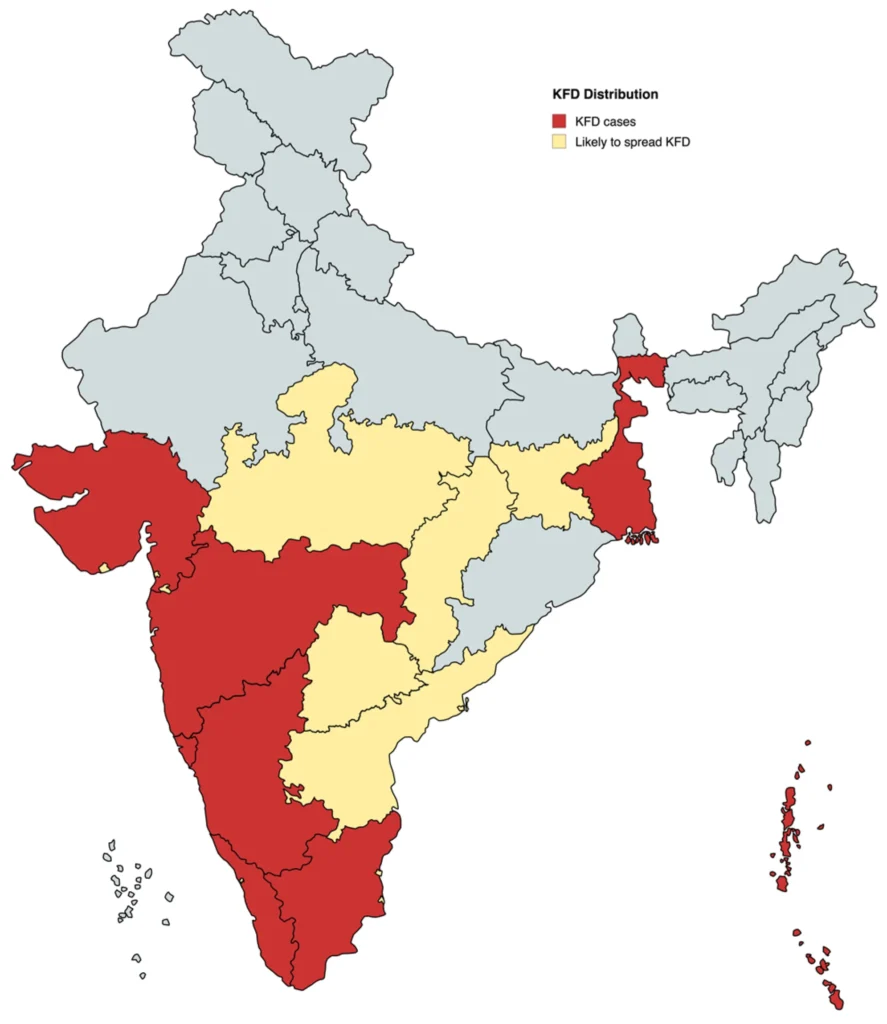
Kyasanur Forest Disease (KFD) is a tick-borne viral haemorrhagic fever primarily reported from southern India. Though geographically limited in comparison to other vector-borne diseases, KFD poses a serious threat to forest-dependent communities, tribal populations, and individuals engaged in agriculture and forestry activities. Its episodic outbreaks and relatively high fatality rate demand sustained public health vigilance.
First identified in 1957 in the Kyasanur Forest area of Karnataka, the disease remains endemic to parts of the Western Ghats region. Despite over six decades of its discovery, KFD continues to challenge health authorities due to ecological complexity, zoonotic transmission, and limited awareness.
Etiology and Virology
KFD is caused by the Kyasanur Forest Disease Virus (KFDV), which belongs to the family Flaviviridae and genus Flavivirus. It is a member of the tick-borne encephalitis (TBE) complex. Viruses within this group are known for causing haemorrhagic fevers and neurological complications.
As a flavivirus, KFDV shares structural similarities with other significant viruses such as dengue and yellow fever. However, unlike mosquito-borne flaviviruses, KFDV is transmitted through ticks, particularly Haemaphysalis species, which act as vectors and reservoirs.
Transmission and Epidemiology
KFD is primarily transmitted through the bite of infected hard ticks, particularly Haemaphysalis spinigera, which act as both vector and reservoir of the virus. These ticks transmit the KFD virus to a range of hosts, including monkeys, rodents, and humans.
The transmission cycle typically operates in forest ecosystems:
- Small mammals such as rodents serve as reservoirs.
- Monkeys act as amplifying hosts, and their deaths often signal an impending outbreak.
- Humans become infected incidentally when they enter tick-infested forest areas.
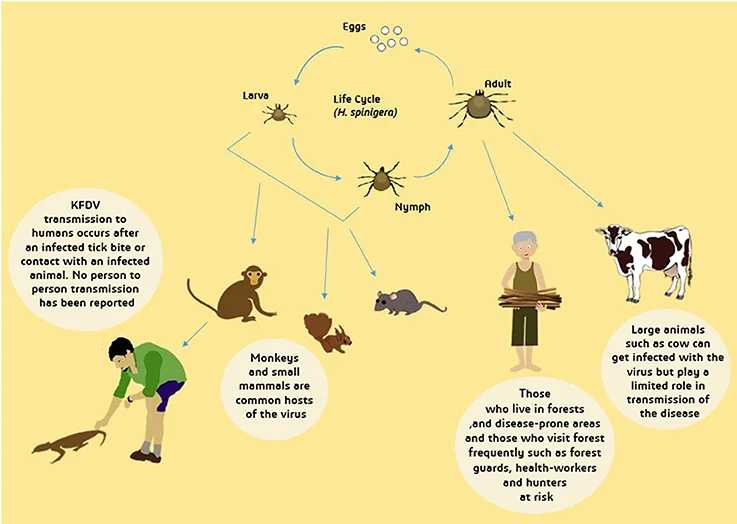
Transmission to humans occurs mainly through:
- Tick bites, especially during forest-related activities such as grazing, firewood collection, or farming near forest fringes.
- Direct contact with infected animals, particularly handling sick or recently dead monkeys.
Importantly, KFD does not spread from person to person, which distinguishes it from many other viral haemorrhagic fevers. The disease follows a clear seasonal pattern. The epidemic period usually begins in October or November, peaks between January and April, and gradually declines by May or June. This seasonal trend corresponds with increased human activity in forest areas and ecological patterns affecting tick populations.
Symptoms
The incubation period of KFD typically ranges from 3 to 8 days after exposure. The disease usually presents with a sudden onset of symptoms, which may include:
- High-grade fever
- Severe weakness (prostration)
- Headache and muscle pain
- Nausea and vomiting
- Diarrhoea
In some patients, the illness progresses to more severe complications, including:
- Neurological symptoms such as confusion or tremors
- Haemorrhagic manifestations, including bleeding tendencies
The case fatality rate is estimated to be between 5% and 10% among known cases, though early detection and treatment can significantly improve outcomes.
Treatment
There is currently no specific antiviral cure for Kyasanur Forest Disease. Management is largely supportive and focuses on reducing complications and stabilising the patient.
Supportive treatment typically includes:
- Maintaining proper fluid balance to prevent dehydration
- Providing oxygen support in cases of respiratory distress
- Monitoring and managing blood pressure
- Treating any secondary bacterial infections
With timely medical intervention and adequate supportive care, many patients recover without long-term complications. However, delayed treatment can increase the risk of severe outcomes.
Conclusion
Kyasanur Forest Disease remains a serious but preventable public health threat in endemic regions. Since there is no definitive cure, emphasis must be placed on early diagnosis, supportive care, vector control, vaccination in endemic areas, and public awareness, particularly among forest-dependent communities. Strengthening surveillance and seasonal preparedness can significantly reduce mortality and contain outbreaks effectively.